We have yet to see the full impact of Covid-19 on waiting lists and the times patients will have to wait for elective surgery. Although there is no question that it has caused a temporary backlog in some areas and for some specialties, we don’t know what the effect will be in the longer term, as we are still working our way out of the pandemic.
Although the focus is, understandably, firmly on the current local and temporary situation, it is also interesting to look at the longer term trends and the international context, as well as the policies different countries have adopted to manage waiting lists.
Even before Covid-19, waiting times were a longstanding concern in many countries, and an OECD report was recently published on the topic. It reviews waiting times across 17 OECD countries, as well as the effect of a range of policies implemented to deal with the issue, using data up to and including 2018-19. A fair comparison One issue when comparing multiple countries is that the definition, the ways of measuring, collecting, structuring and reporting on the data varies between countries, limiting comparability.
Waiting times, for example, can be recorded from the GP referral or following a specialist visit. Some health systems will measure the “outpatient” waiting time, others the “inpatient” waiting time, yet others measure the full referral-to-treatment waiting time, as is the case in Denmark, Norway and England.
While the mean and the median waiting time, waiting time at certain percentiles of the distribution - and the number or proportion of patients waiting more than a threshold period of time (e.g. 3, 6 or 12 months) - are all valid ways of measuring waiting times, the median is most commonly used for international comparisons.
However, the distribution of waiting times is generally skewed with a small proportion of patients waiting a very long time, meaning the mean waiting times can be substantially longer than the median. How do OECD countries compare? The OECD study shows that waiting times for elective surgery can vary widely between countries, with waiting times almost 10 times higher in some countries than others.
Data on waiting times are currently available only for 17 OECD countries and for certain procedures. On average across these countries, the median waiting times were shorter for more minor surgery, such as cataract operations (95 days in 2018), and longer for more major surgery like hip replacement (110 days) and knee replacement (140 days).
In all countries, patients requiring more urgent treatments generally have a shorter wait than those whose health status is less likely to deteriorate while waiting. Therefore, median waiting times for coronary bypass surgery are generally shorter than for hip and knee replacement.
However, there are huge variations across countries. Overall, waiting times for elective surgery in 2018 were the lowest in Denmark, the Netherlands, Italy and Hungary, while they were the highest in Estonia, Poland and Chile.
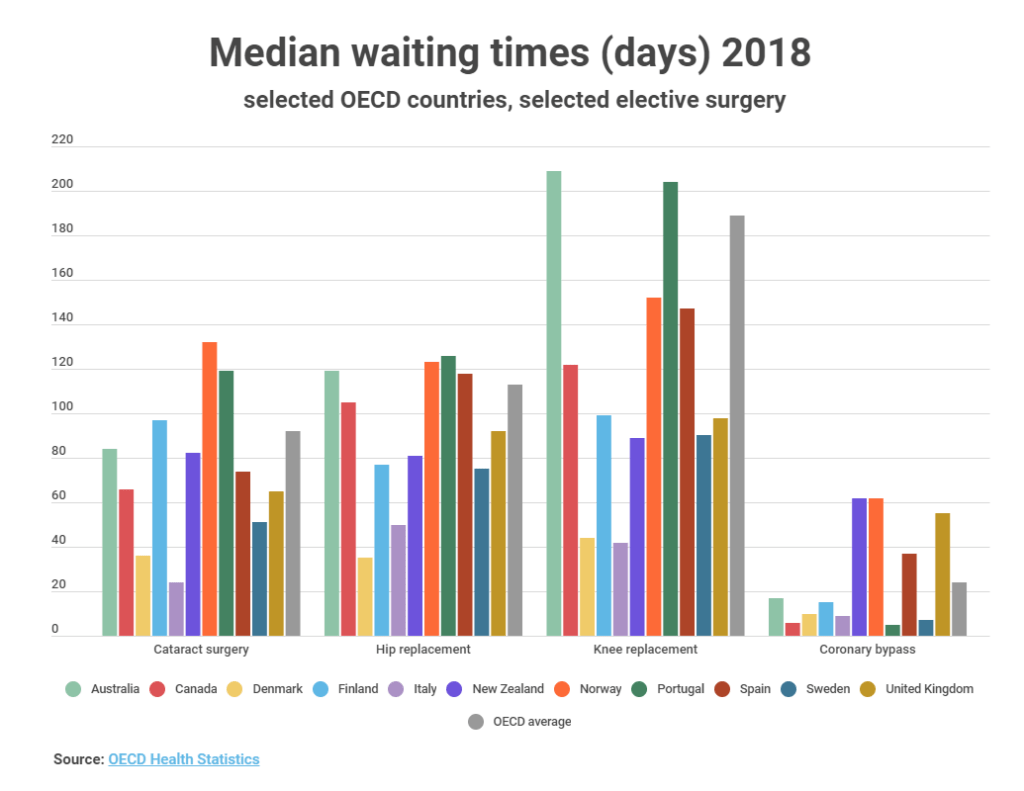
The chart below shows the median waiting times for some selected OECD countries with comparable data for different types of surgery.
As the chart shows, the median waiting times for cataract surgery were highest in Norway, Portugal and Finland. It should be noted, however, that two countries not shown in this chart - Estonia and Poland - had significantly higher waiting times at 180 and 250 days respectively. Norwegian waiting times are also calculated in a slightly different way. The majority of countries included in the chart had waiting times lower than the OECD average with Italy, Denmark and Sweden recording some of the shortest waits.
For hip replacements, the picture was similar and many countries recorded long waits for hip replacements. However, Spain and Canada had high median waiting times, and the wait in Australia was also above the OECD average, and significantly above the New Zealand median.
Along with Portugal, Australia also stands out for its waiting time for knee replacements; one of the highest out of all OECD countries at more than 6 months. The OECD average is high for this type of procedure and was brought up by relatively few countries with very high waiting times, such as Chile, which has a median wait of 840 days, and Estonia with 460 days.
 How have waiting times changed over time?
The OECD figures show that, following a period of stability, waiting times for elective treatment (which are usually longest) had started to rise in a number of countries, even before the Covid-19 outbreak.
How have waiting times changed over time?
The OECD figures show that, following a period of stability, waiting times for elective treatment (which are usually longest) had started to rise in a number of countries, even before the Covid-19 outbreak.
However, changes to the median waiting time in countries such as United Kingdom and Australia have been relatively small from an international perspective compared to, for example, Estonia and Portugal.
Many countries have implemented policies focused on reducing waiting times, with mixed results. Denmark, England and Finland have succeeded in reducing waiting times for many elective health services and maintained these over sustained periods, and as shown in the charts, Poland has managed to reduce waiting times substantially within the last five years.
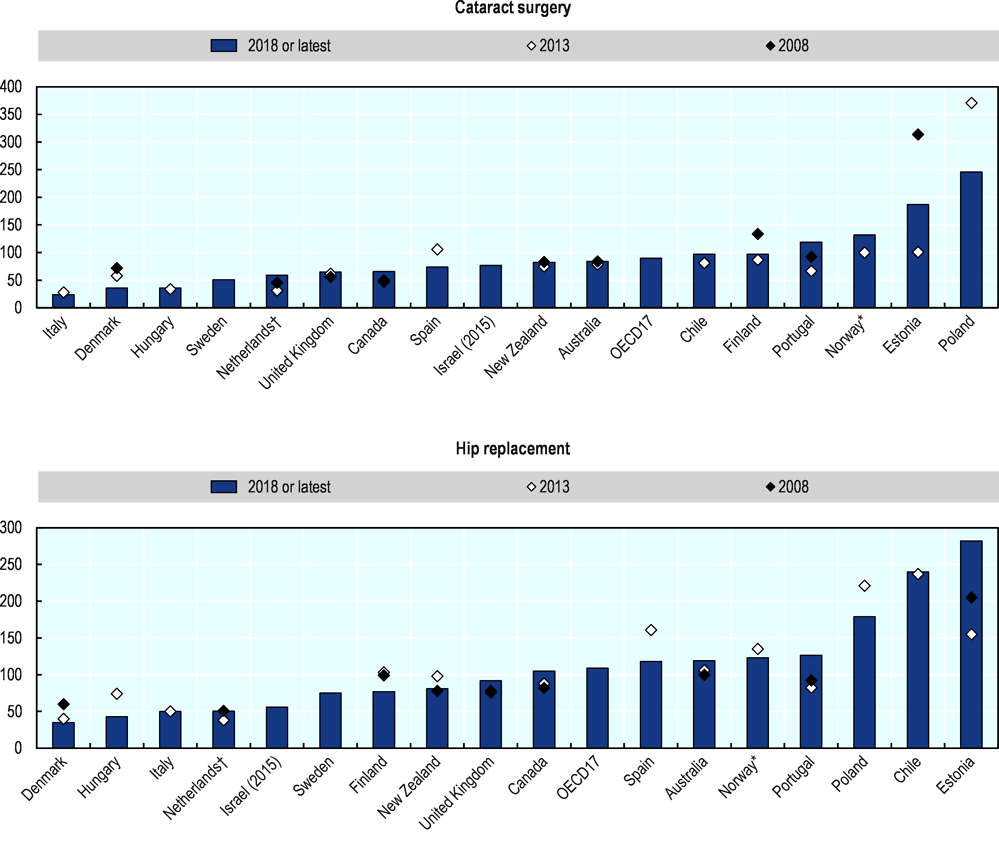 Note: † For the Netherlands, the data is the mean, because the median is not available * For Norway, waiting times are over-estimated due to the way waiting times are calculated.
Source: OECD Health Statistics
How are waiting times addressed in different countries?
When waiting lists arise, it is generally the result of an imbalance between the demand for and the supply of health services. The right policies to implement will be different in each country and depends on the health system, the financial and political situation among other factors.
Note: † For the Netherlands, the data is the mean, because the median is not available * For Norway, waiting times are over-estimated due to the way waiting times are calculated.
Source: OECD Health Statistics
How are waiting times addressed in different countries?
When waiting lists arise, it is generally the result of an imbalance between the demand for and the supply of health services. The right policies to implement will be different in each country and depends on the health system, the financial and political situation among other factors.
Maximum waiting times have been used in many countries as a target for providers, and in some cases a guarantee for patients, but there is no “one-size-fit-all” maximum waiting time.
Permanent and sustained increases in supply are the most effective way to achieve permanent reductions in waiting times. However, short-term interventions using occasional additional funding packages also serve an important purpose. By quickly responding to a temporary increase in demand or a short-term disruption in supply, waiting lists can be prevented from rising substantially and causing a backlog, and causing increased waiting times further down the line or over a longer period of time.
Even permanent increases in supply are not a guarantee of success. In some cases additional supply can be offset by an increase in demand, through an increase in referrals, tests and procedures. For example, waiting times for some elective surgery in Canada and Australia have increased in recent years despite additional funding and an increase in activity.
In Australia, the investment in elective surgery under the 2011-15 National Partnership Agreement meant the growing demand could be met, but did not lead to a significant impact on waiting times. Between 2015 and 2018, waiting times for cataract surgery had declined slightly, but had increased slightly for knee replacement and hip replacement.
Where there is substantial excess demand, the demand side is also sometimes targeted in order to reduce waiting times. Clinical prioritisation tools that focus on improving health outcomes can improve the referral process and the management of waiting lists.
In the OECD report, New Zealand is used as an example of a country that has tried to improve the prioritisation of patients (but in combination with increasing supply). Following a reduction in waiting times for elective surgery to a maximum of 4 months in 2012, waiting times have declined for many common procedures and are well below OECD averages.
Since 2019, the New Zealand Ministry of Health is implementing a broader approach with a focus on the whole patient pathway under its ‘Planned Care Strategic Approach 2019-2024’. The impact on access to care and health outcomes A large amount of evidence points to the fact that long waiting times can have negative effects on both access to care and health outcomes for patients. This is a concern with addressing waiting lists on the demand side by rationing waiting times and implementing prioritisation policies.
Patients’ conditions can deteriorate during the wait, especially if the wait is extended or the patient de-prioritised. Although the need for a hip replacement, for example, is not life threatening, living with such a condition long term is debilitating and can reduce the patient’s quality of life substantially.
As well as having potentially serious consequences for patients and being a source of unmet care needs in some countries, long waiting times can also result in inequalities in access. Ideally, access to care should be based on need and not ability to pay.
Some patients will inevitably have more options than others, and on an international basis, there are vast inequalities in access depending on where the patient lives. For example, the maximum waiting time for a cataract surgery ranges between countries from one month in Denmark to 1.5 years in Estonia. Even within a country, there can be substantial differences between access in rural and metropolitan areas.
It is also likely that the Covid-19 pandemic will have impacted very differently on health systems in different countries, but more data is needed to understand this. What can be done to improve waiting times? Although they vary, the fact is that waiting lists, and therefore waiting times, have increased substantially in many countries over the last decade. Covid-19 is also having a detrimental impact on waiting times, with expected recovery hampered by a second and third wave.
To address this, there is a need to substantially expand capacity – and to do this quickly. One way to quickly and efficiently increase capacity is to use flexible healthcare infrastructure, such as mobile or modular operating theatres .
A temporary room can be in place for a longer period to cover works to expand the existing department, or for a shorter period to boost activity and ‘blitz’ waiting lists that have built up over time. Such a solution can be set up as a dedicated stand-alone unit for high-volume surgery, having minimal impact on the hospital’s existing resources. A range of flexible solutions are available from Q-bital Healthcare Solutions .
Other strategies are aimed at improving the coordination between primary and secondary care, which can provide better patient flow and valuable insight into the entire patient pathway and waiting times at each stage of the journey. Flexible healthcare can help with this too; for example, a mobile or modular minor injuries clinic can be placed adjacent to the hospital’s main A&E department to help direct patients into the most suitable pathway.
Ultimately, reducing the time that people have to wait for access to health services is essential to improving the patient experience - a key priority in most countries.
Q-bital Healthcare Solutions
Unit 1144 Regent Court, The Square, Gloucester Business Park, Gloucester, GL3 4AD